現在位置 : 經濟 > 美國醫療費用世界最昂貴 - Most Expensive, US Medical Cost
|
美國醫療系統 (US Medical System)
美國醫療系統是由許多個合法個體提供的醫療服務業。美國的醫療設施和醫療保險大部分都由私營部門經營,美國政府會提供較為輔助性質的公共醫療保險、醫療輔助計畫、小童醫療保險計畫和榮民(退伍軍人)健康管理。歐盟和美國的藥業組織認為美國是全球醫學研究及推出新型醫術和醫療產品的龍頭國,她們又表示必須依靠美國高昂的醫療開支才能有效推動這些研發的進行。"世界衛生組織"(WHO)在2000年的世界衛生報告中比較了191個成員國的醫療質素,美國的醫療消費與應變能力都在榜首、總體衛生系統表現排第37位、總體人口健康程度排第72位。2008年美國聯邦基金比較19個已發展國家的醫療系統質量,美國排名榜尾。 2007年至2008年的統計顯示,最少有15%的美國國民得不到任何醫療保險計劃的保障,另外還有很大部分的美國國民購買的醫療保險未能有效保障其受益人。而美國個人醫療費用開支是全世界最昂貴:根據經濟合作與發展組織(OECD)以購買力平價計算,美國2007年的人均醫療開支為7,290美元、佔國內生產總值(GDP)16%,這兩項數據都是全球最高的。龐大的個人醫療支出引致了巨額的醫療貸款,而所導致的個人破產就佔了全美國破產個案的62%,但當中75%的申報破產人士已投保醫療保險。美國國家科學院醫學研究所2004年就發表過美國是個富裕而已工業化的國家,但美國政府還未能擔保全國人民獲得醫療保險的保障,因此每年約有1萬8千名美國國民死於缺乏醫療保險。而哈佛醫學院2009年發布的死亡數字比醫學研究所的更高,是每年44,800人。 |
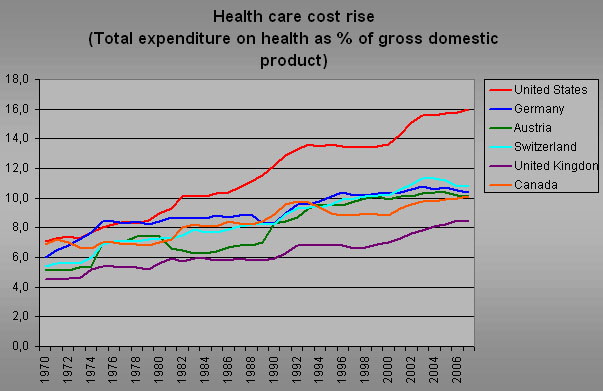
OECD統計- 1970年-2007年美國、德國、奧地利、瑞士、英國和加拿大的醫療開支比GDP的圖表 --US Health care cost on the rise
|
|
美國醫療設施
在美國,由慈善或宗教團體經營的非牟利醫院佔了主流,其次為地方政府醫院和私營牟利醫院,2003年它們的比重約為62%-20%-18%。聯邦政府本身營運的全國性保健系統並不對外開放,它們分別是由國防部管理的軍用醫療系統及為退伍軍人提供保健服務的榮民健康管理局。印第安人保健服務所(IHS,直屬於衛生及公共服務部)就只提供醫療服務給印第安及阿拉斯加原住民使用,亦會以合約形式僱用私家醫療服務團體專為他們提供保健服務。面向一般民眾的非牟利醫院雖然可以獲得政府免稅,但它們依然會對病人收取高昂的醫療費用,對沒投保健保的病人更甚,亦引起了對這些醫院的經營道德爭議和法律訴訟。 醫院雖然會提供急診和門診服務,但它們都主要為住院病人而設。另類的專科診所有「手術中心」(surgicenter)專為客人提供手術後不需住院療養的即日服務、善終收容所為預計剩餘壽命少於6個月的末期病患者提供臨終關懷服務等。 個人醫療支出 2006年美國的醫療支出佔國內生產總值(GDP)大約15到16%,在所有聯合國的成員國中僅次於東帝汶的大約18%;這支出有31%流到住院療養、21%歸內科服務、10%花在購買藥物、8%護老服務、7%屬行政費用和23%歸入其他項目裡,包括實驗室診斷服務、製藥業、醫療器具生產商等等。美國醫療保險和醫療補助服務中心的會計部比較每年的醫療支出數字,2008年的國民總醫療支出為2.34萬億美元,比較往年增長4.4%,增長速度維持在6%左右的水平,人均醫療開支為7,681美元,醫療支出比GDP為16.2%,年度升幅在0.1%到0.3%之間浮動。美國衛生及公共服務部預計若繼續維持2008年的醫療體制,到2017年醫療支出比GDP會上升到19.5%,比醫療保險和醫療補助服務中心預計的數字要高一點。2010年3月,股神巴菲特就評價過,美國公司為其僱員支付的醫療開支使它們處於競爭劣勢:以GDP的17%消費在保健上但偏低的醫護人員與國民比例,對照其他大部分國家的平均9%而言,就像一條絛蟲蠶食著美國的經濟體系。 |
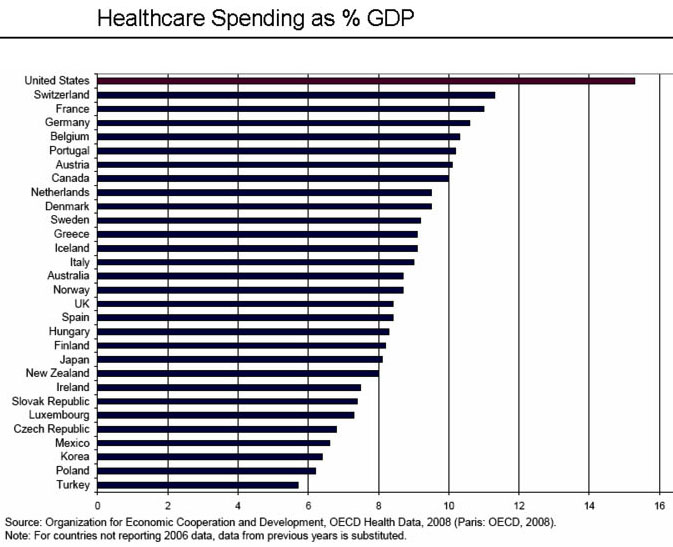
OECD2008年統計- 醫療開支佔30國GDP比例,美國排名榜首 International Comparison - Healthcare spending as % 25 GDP
|
|
美國健保危機
七十萬美國人宣告破產的背後原因是? 紀錄片【美國健保危機】告訴你! 你可能不知道全世界最富強的美國,沒有健保制度。美國人民因此被迫為了健保福利而找工作;甚至為了健保無法結束婚姻關係,又稱做"婚姻鎖定",為了公司提供的健保而不願退休。 • 為了健保而工作 • 為了健保而不離婚 • 為了健保而不退休 美國以營利為目的的健康保險 在私人市場中沒有人能逃過醫療審核的魔掌。保險公司藉由醫療審核挑選健康保戶,淘汰病患。拒保的原因包括花粉熱、青春痘。有人被拒保是因為他們超重了20磅,有的小孩子是因為尿床或有中耳炎。這些常見的小毛病,在美國人民想買核保保單時都會造成問題。 美國既得利益者防堵全民健保的推動! 美國價值2.2兆的健保體系,充斥著既得利益者(私營保險公司)、利益關係人(醫生、醫院)和說客等等。還沒碰過一個覺得自己賺太多的醫師,而是認為自己賺得太少;沒碰過一個覺得可以不用這麼多錢就能維持醫院營運的醫院主管。沒碰過一個願意犧牲醫療照顧的病人,每一個病人都覺得優質照顧等同於讓他們要什麼有什麼;沒碰過任何一個願意少拿一點的人。 美國前第一夫人希拉蕊曾在柯林頓總統任內,企圖推動美國全民健保,卻無功而返。現在歐巴馬沉重的呼籲:「保健改革不能等也不可以等!」 |

位於美國洛杉磯的凱薩日落醫院 (Kaiser Sunset Hospital)
|
|
● 美國歐巴馬總統企圖推行全民健保,通過健保法案,但仍面臨一些困難
Obamacare, The Affordable Care Act (ACA) The Patient Protection and Affordable Care Act (PPACA), commonly called Obamacare or the Affordable Care Act (ACA), is a United States federal statute signed into law by President Barack Obama on March 23, 2010. Together with the Health Care and Education Reconciliation Act, it represents the most significant regulatory overhaul of the country's healthcare system since the passage of Medicare and Medicaid in 1965. The ACA aims to increase the quality and affordability of health insurance, lower the uninsured rate by expanding public and private insurance coverage, and reduce the costs of health care for individuals and the government. It provides a number of mechanisms - including mandates, subsidies, and insurance exchanges - to increase coverage and affordability. The law also requires insurance companies to cover all applicants within new minimum standards and offer the same rates regardless of pre-existing conditions or sex. Additional reforms aim to reduce costs and improve healthcare outcomes by shifting the system towards quality over quantity through increased competition, regulation, and incentives to streamline the delivery of health care. The Congressional Budget Office projected that the ACA will lower both future deficits and Medicare spending. On June 28, 2012, the United States Supreme Court upheld the constitutionality of most of the ACA in the case National Federation of Independent Business v. Sebelius. However, the Court held that states cannot be forced to participate in the ACA's Medicaid expansion under penalty of losing their current Medicaid funding. Since the ruling, the law and its implementation have continued to face challenges in Congress, in federal courts, and from some state governments. |
US President Obama portrait crop
|
|
(Looking for Answers)
What's The Most Expensive Medical Condition? November 3rd, 2009 by Toni Brayer, M.D. in Better Health Network What medical condition costs the U.S. Health system the most in disability and overall costs? If you said heart disease or cancer or pulmonary disease you would be wrong! I would have said one of those myself. The answer…slow drumroll….is musculoskeletal disease. Yes, 50% of the adult population reported having a disabling musculoskeletal condition in 2008. The expenditures for these problems include the costs of preventive care, the cost of direct care, the cost of care in hospitals, by physicians, therapists and other caregivers. It also includes the loss of productivity. In 2004 it was estimated that the cost of care for musculoskeletal problems was $840 billion. (Hey, isn’t that about equal to the bank bailout?) What are musculoskeletal conditions? They include that old nemesis: Low back and neck pain. Spine problems are among the most common problems that bring patients for medical care. That’s why the chiropractic industry is booming. Another leading cause of disability is osteoarthritis, which affects almost 22% of all adults. Osteoarthritis leads to millions of Advil and Tylenol doses and often culminates with total joint replacement (hips and knees). With the influx of baby boomers, the increase in total joints will ensure orthopedic surgeons decades of future employment. Osteoporosis (bone loss) is another disease of aging that causes hip, spine and humerus fractures in people older than 65. All of those Sally Field commercials for Boniva are aimed at consumers and the expense to diagnose and prevent bone loss adds to the overall cost of treatment. About 60% of all injuries involve the musculoskeletal system and falls are the most common cause. The emergency department, doctors offices and hospitals all deal with patients with bone and muscle injuries. Patients that are admitted to a hospital spend an average of 5 days in the hospital. Ching, ching! Despite these facts, the NIH research budget for musculoskeletal conditions has been decreasing with time and they are not in the top 10 conditions that receive funding. In addition, the proportion of orthopedic surgeons to the aging population is not keeping pace. We aren’t training enough orthopedic surgeons to keep up with demand and the projected need for 2020 is woefully short. With declining Medicare payments and rising malpractice insurance costs, physicians are shying away from specialties that take care of “old” people. Rheumatology, geriatrics, primary care and orthopedic surgery are all specialties that are going to be needed, but we have done no workforce planning as a nation to ensure there will be enough to care for the population. |
