現在位置 : 檢查 > 胸部X光檢查 Chest X-ray
Chest X-ray
|
|
Chest X-ray
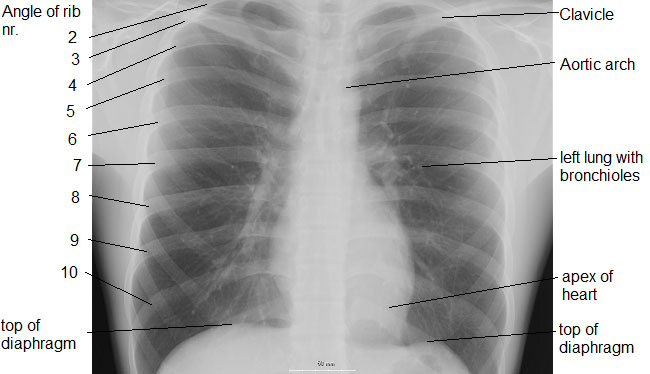
In medicine, a chest radiograph, commonly called a chest X-ray (CXR) or chest film, is a projection radiograph of the chest used to diagnose conditions affecting the chest, its contents, and nearby structures. Chest radiographs are among the most common films taken, being diagnostic of many conditions. Like all methods of radiography, chest radiography employs ionizing radiation in the form of X-rays to generate images of the chest. The mean radiation dose to an adult from a chest radiograph is around 0.02 mSv for a front view (PA or posterior-anterior) and 0.08 mSv for a side view (LL or latero-lateral). Problems identified Conditions commonly identified by chest radiograph Pneumonia Pneumothorax Interstitial lung disease Congestive heart failure Bone fracture Hiatal hernia Chest radiographs are used to diagnose many conditions involving the chest wall, including its bones, and also structures contained within the thoracic cavity including the lungs, heart, and great vessels. Pneumonia and congestive heart failure are very commonly diagnosed by chest radiograph. Chest radiographs are used to screen for job-related lung disease in industries such as mining where workers are exposed to dust. For some conditions of the chest, radiography is good for screening but poor for diagnosis. When a condition is suspected based on chest radiography, additional imaging of the chest can be obtained to definitively diagnose the condition or to provide evidence in favor of the diagnosis suggested by initial chest radiography. Unless a fractured rib is suspected of being displaced, and therefore likely to cause damage to the lungs and other tissue structures, x-ray of the chest is not necessary as it will not alter patient management. The main regions where a chest X-ray may identify problems may be summarized as ABCDEF by their first letters: Airways, including hilar adenopathy or enlargement Breast shadows Bones, e.g. rib fractures and lytic bone lesions Cardiac silhoutte, detecting cardiac enlargement Costophrenic angles, including pleural effusions Diaphragm, e.g. evidence of free air, indicative of perforation of an abdominal viscus Edges, e.g. apices for fibrosis, pneumothorax, pleural thickening or plaques Extrathoracic tissues Fields (lung parenchyma), being evidence of alveolar flooding Failure, e.g. alveolar air space disease with prominent vascularity with or without pleural effusions Views Different views (also known as projections) of the chest can be obtained by changing the relative orientation of the body and the direction of the x-ray beam. The most common views are posteroanterior, anteroposterior, and lateral. In an posteroanterior (PA) view, the x-ray source is positioned so that the x-ray beam enters through the posterior (back) aspect of the chest, and exits out of the anterior (front) aspect where the beam is detected. To obtain this view, the patient stands facing a flat surface behind which is an x-ray detector. A radiation source is positioned behind the patient at a standard distance (most often 6 feet), and the x-ray beam is fired toward the patient. In anteroposterior (AP) views, the positions of the x-ray source and detector are reversed: the x-ray beam enters through the anterior aspect and exits through the posterior aspect of the chest. AP chest x-rays are harder to read than PA x-rays and are therefore generally reserved for situations where it is difficult for the patient to get an ordinary chest x-ray, such as when the patient is bedridden. In this situation, mobile X-ray equipment is used to obtain a lying down chest x-ray (known as a "supine film"). As a result, most supine films are also AP. A chest radiograph with the angle parts of the ribs and some other landmarks labeled. Lateral views of the chest are obtained in a similar fashion as the posteroanterior views, except in the lateral view, the patient stands with both arms raised and the left side of the chest pressed against a flat surface. Typical views In the United States, initial imaging of the chest generally consists of PA and lateral views. In other countries, the PA view suffices as an initial study; the lateral view is only added if indicated from reading of the PA view. Additional views Decubitus - useful for differentiating pleural effusions from consolidation (e.g. pneumonia) and loculated effusions from free fluid in the pleural space. In effusions, the fluid layers out (by comparison to an up-right view, when it often accumulates in the costophrenic angles). Lordotic view - used to visualize the apex of the lung, to pick-up abnormalities such as a Pancoast tumour. Expiratory view - helpful for the diagnosis of pneumothorax. Oblique view |
Chest X-ray
|
